Fresh Look: AAC for Children Who Have Rett Syndrome with Dr. Theresa Bartolotta
In our SLP training programs, few of us learned about Rett Syndrome or how to provide services to children with that disorder. We’re so pleased to have a guest post on AAC services for children with Rett by Dr. Theresa Bartolotta, Director of Assessment in the Office of the Provost, and Associate Professor in the Department of Speech-Language Pathology, at Seton Hall University, in South Orange, New Jersey. An SLP with over 30 years of clinical experience, she specializes in communication disorders in children with significant disabilities with a special interest in autism and Rett syndrome. Our field is still learning about Rett syndrome and we are still discovering new things about the range of skills and abilities present in the children who have it. In this post, Dr. Bartolotta gives us some background about the syndrome and discusses implications for treatment.
I am thrilled to have this opportunity to post about Rett syndrome, and share some strategies on successful use of AAC with individuals with Rett on this blog!! Thanks to Carole Zangari for this gracious invitation.
Background
I began working with individuals with Rett syndrome (RTT) about 15 years ago, and at that time, there was very little information available for clinicians, teachers and families regarding best practices in working with this population. Rett Syndrome was initially described in the 1960’s in Europe, and the first individual with RTT was diagnosed in the U.S. in the 1980’s. A fairly rare disease, it occurs in approximately 1:10,000 live female births, but is the second-most common cause of severe intellectual disability in females. RTT does occur in males, though less frequently than females, and most times the males are very severely affected.
So – why is there so much interest in RTT and why are more and more clinicians seeing cases of RTT?
Genetic Cause
The genetic mutation that causes RTT was identified in 1999 and as a result, a great deal of interest in the disorder has been generated since that time. RTT most commonly occurs as a spontaneous mutation on the X chromosome in the MECP2 gene. This gene plays a major role in the development of the brain and in healthy brain function throughout the lifespan. At present there are countless studies underway to learn more about this very complex gene, and more importantly, to identify clinical treatments, and eventually, a cure. The diagnosis of RTT is made clinically, typically by a developmental pediatrician or neurologist, and then confirmed through a blood test. Many early cases of RTT are initially misdiagnosed as autism, especially when the signs of the disorder first become apparent. Until recently RTT was considered to be part of the autism spectrum, but with the release of the new DSM 5 this year, it is no longer listed as an autism spectrum disorder.
The finding of the gene has resulted in more accurate diagnosis of RTT and better understanding of the challenges faced by individuals and their families. As recently as 10 years ago, individuals with RTT were believed to be incapable of intentional communication and likely faced the loss of all motor skills at an early age, and an early death. We now know this is not the case. It is not a degenerative disorder. Many individuals with RTT live well into middle age, retain walking skills and some hand function and participate in their community. We are beginning to learn about the variations in cognitive and communication ability as well. Though most individuals are severely cognitively challenged, nonverbal, and dependent for self-care, they tend to be very social and interested in people and various activities. The key challenge is how to identify the best way for the individual to communicate and to maximize their potential.
Characteristics of RTT
Individuals with RTT have severe challenges in cognition, communication and motor function. Here are some key facts:
- Symptoms usually appear between six-18 months of age
- Most infants with RTT appear to function normally until experiencing a regression in motor skills, language and cognition sometime before the second birthday
- The period of regression can last for several years
- Most individuals can then regain skills, or learn some new skills, in later childhood through adulthood
- Seizures, respiratory, and feeding problems are often present
- Hand function is usually very limited
- Apraxia is commonly observed and affects most body movements
- The overwhelming majority will be nonverbal and not develop functional spoken language skills
- Many individuals with RTT have excellent eye gaze – this modality has strong potential for communication
- Early intervention with AAC can assist in development of communication and cognitive skills and improve quality of life for those with Rett syndrome
Assessment of Communication
Because of the complexity of the disorder, standardized tests usually do not provide the most functional, clinically applicable or relevant information for clinicians to identify the best approach to designing communication intervention. Two tools which I recommend are The Inventory of Potential Communicative Acts (IPCA) (Sigafoos et al.,2006) and The Communication Matrix (see references at the end). Each of these tools use a series of questions to gather information from a communication partner of the individual you are assessing. These are highly functional ways to gather useful information about communication and social behaviors of individuals who are at a prelinguistic or early linguistic level of communication development.
Communication Intervention
Most individuals with RTT will not develop functional verbal skills. So, for this population, implementation of AAC strategies EARLY will help provide the best outcomes. Volitional hand control is usually limited because of severe difficulties with apraxia. They often need additional time to generate a response, so keep that in mind when asking questions or giving a command.
Many individuals with RTT use nonstandard behaviors for communication. For example, to make a request, a person with RTT may walk towards or lean towards an object. Some of the behaviors to be on the lookout for are: vocalizations, laughing, crying, eye gaze, head or body movements. These nonstandard behaviors are often described as prelinguistic, in that they don’t fit the criteria for symbolic communication, but if acknowledged as communicative or potentially communicative, a meaningful, symbolic act can be shaped. The communication partner, someone who is familiar with the individual with RTT, can provide an abundance of information about interests and help you interpret the meaning of these behaviors.
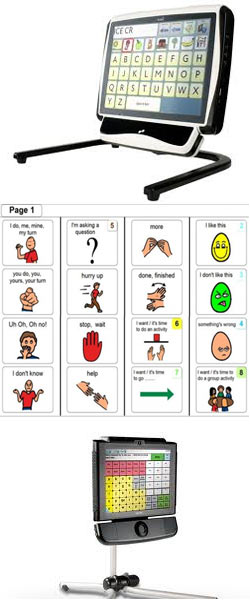
Consideration of alternative access for AAC using body parts other than the hands, including head, arm, or eyes should be a primary goal. Persons with RTT are often described as making consistent eye contact with others, so this is a good modality to begin to explore. There’s lots of interest at present in using electronic eye gaze systems, and there’s some excellent research that demonstrates individuals with RTT have gaze patterns similar to typically developing children (Djukic & McDermott, 2012; Djukic et al, 2012). However, before making significant investments of time, money and other resources in electronic systems, you may want to consider trying to utilize low-tech or no-tech eye gaze options, using partner-assisted scanning.
Here are some ideas for Best Practices in AAC Intervention for RTT:
- Begin by teaching a simple requesting response
- Ensure the targeted response is within the individual’s physical abilities – consider nonstandard behaviors
- Consider a simple motor act rather than speech or gestures
- Touch a switch
- Hand movement
- Natural gesture
- Assess use of eye gaze
- Offer choices
- Develop consistency across two favored objects
- Explore expanding set to three or more choices
- Begin with no-tech; establish a consistent, valid level of response
- However, allow for inconsistency (remember – apraxia can affect consistent motor responses)
- Allow time to respond – many individuals with RTT have delayed responses – asses an individual and adjust your expectations
- Move to low-tech or high-tech, depending upon:
- Interest level
- Skill
- Resources
- Contexts
Specific Interventions
The evidence for successful use of AAC with RTT is limited, but here are some techniques that are discussed widely in the RTT community:
- Communication Coaching –See Bartolotta & Remshifski (2013) for more information.
- The communication partner is the best resource to interpret what behaviors mean
- Coaching is highly effective in terms of SLP time and resources
- You can implement any type of AAC strategy into a coaching model
- How to do it:
- Observe an interaction between an individual with RTT and a familiar person
- Provide targeted strategies to implement during familiar settings, such as:
- Offer choices
- Increase wait time to allow for responses
- Acknowledge behaviors that can be potentially communicative
- Eye gaze, open mouth, vocalization, hand and body movements
- Ask questions or make comments that require responses
- PODD
- Pragmatic Organization Dynamic Display Communication Books – developed by Gayle Porter
- Provides guidelines and templates for communication books
- Contains tips for teaching strategies and how to choose relevant, motivating vocabulary
- Books can be accessed using direct selection, scanning, partner-assested scanning
- Available from Mayer-Johnson (www.mayer-johnson.com)
- See Linda Burkhart’s website for information on training opportunities for PODD
- Electronic eyegaze systems
- Infrared cameras provide access to a range of devices using eyegaze
- Very population devices: Dynavox Eyemax, TobiiC12 or C15 Communicators
- Emerging interest in using this type of AAC strategy given the strong eye gaze modality we observe in those with RTT
- Suggestions for implementation
- First establish consistent eye gaze using high-interest objects, photos or symbols
- It can be very challenging to achieve calibration for individuals with RTT – go slow, and don’t be discouraged. It takes time to learn how to activate buttons using eyegaze
- Begin slowly using high-interest activities
- Trial a device before recommending a purchase (as you would with other clients)
- Remember that one system won’t work in all contexts, so explore multiple communication options
Working with individuals with RTT and their families can be challenging yet highly rewarding! We can learn so much about alternative ways to meaningful communication with this population. As one family said, “these girls have so much to say if we only listen”.
Any questions – please contact me at: theresa.bartolotta@shu.edu
References/Resources
Bartolotta, T.E. & Remshifski, P.A. (2013). Coaching communication partners: A preliminary investigation of communication intervention during mealtime in Rett syndrome. Communication Disorders Quarterly, 34(3), 162 – 171.
Communication Matrix – http://www.communicationmatrix.org
Djukic, A. & McDermott, M.V. (2012). Social preferences in Rett syndrome. Pediatric Neurology, 46, 240-242.
Djukic, A., McDermott, M.V., Mavrommatis, K., & Martins, C.L. (2012). Rett syndrome: Basic features of visual processing – a pilot study. Pediatric Neurology, 47, 25-29.
International Rett Syndrome Foundation – http://www.rettsyndrome.org
Sigafoos, J., Arthur-Kelly, M. & Butterfield, N. (2006).Enhancing everyday communication for children with disabilities. Baltimore, MD:Brookes.

Filed under: PrAACtical Thinking
Tagged With: eye gaze, Rett syndrome, RTT, Theresa Bartolotta
This post was written by Carole Zangari

19 Comments
I work with a wonderful young lady with Rett’s Syndrome. She seems to defy all the literature, and has great hand control. Using AAC with her has been wonderful. She is so socially motivated, and is really showing her team what she can do. We started small, with just one picture, but now she is able to scan a page full of pictures and get the one she wants. Next step- a dynamic device. Starting slowly was the key, and it was worth it, as we are seeing all sorts of growth from this young lady.
That’s awesome, Jennifer! It serves as one more reminder that we have so much yet to learn about this syndrome and that we have to keep setting the bar high. Thanks for stopping by and sharing this!
Jennifer – thanks for sharing! So glad to hear that you are seeing progress with this young woman. I agree, starting slowly is so important, so you can figure out what works and you both can move in a positive direction. We are seeing so much variation in the syndrome, so what was previously reported in the literature is not always the most valid information for your individual client. Your comment about hand control is one example. Best of luck!
Thanks for sharing this! What a great post for parents, teachers, and therapists new to Rett syndrome.
I hope you don’t mind that I shared this in a post over at my blog, since a number of Rett parents check in there. I’m eager to send them your way, not only for Dr. Bartalotta’s article but also the other fantastic information you so generously share.
Rose-Marie, we are huge fans of your blog and are delighted that you wanted to share this post. Thank you!
Rose-Marie – thanks! I checked out your blog – great information. I greatly appreciate you sharing this post.
Wow that was odd. I just wrote an extremely long comment but after
I clicked submit my comment didn’t show up. Grrrr… well I’m not writing
all that over again. Anyway, just wanted to say wonderful
blog!
Hi Theresa, what a great article about Rett Syndrome – an introduction to the medical background for those who need the updated version, information about assessment techniques, and plenty of very practical ideas for intervention (AAC). We need to get this information “out there” to inform practice and support to the girls (and boys) with RTT.
Dear all,
I will be getting a class with five young ladies with Rett next year. I will be receiving training in the fall on the My Tobiis. However, I would love to learn more on how to use the devices before that, so I can be of assistance immediately when school starts. Does anyone know of a way I can receive instruction before school starts? Please let me know, blessings, Nancy
Nancy, good for you for reaching out! I would check out what the company offers online (e.g., http://praacticalaac.org/praactical/teach-me-tuesday-tobii-c-8/). Also, there are some terrific Rett Facebook groups for families, educators, and other professionals. You might want to join some of them to post this question. This post went live a year ago and I am not sure how many people will respond here. Just a thought.
Hello everyone,
I am getting five young ladies who are in their mid teens next fall. I will not be trained on the My Tobiis until the fall. I need to receive instruction before that, does anyone know of a place I can go and take a course, even if it is on the computer? I live in NY. Please advise.I have two books coming on Rett, and excellent resources. However, I want to know how to teach in a way that gives these students my best, so scheduling is important too. What are other teachers out there with Rett students focusing on? Many thanks in advance, Nancy
Hi Nancy – good for you, getting this kind of preparation done ahead of time! There are lots of people around the world who have expertise in Rett Syndrome, and Theresa is one of those people, so glad you found her article.
Training can be provided by Tobii if you contact your local Tobii Rep for NY area, but they have lots on information online, e.g. http://www.tobii.com/en/assistive-technology/global/support-and-downloads/ and
http://www.tobii.com/en/assistive-technology/north-america/training/
There are a few other things I can recommend:
1. Please request join my closedProfessionals group on Facebook for clinicians and teachers who are working with people with RTT: https://www.facebook.com/groups/493049477417482/
2. You could also request to join the closed Facebook page: https://www.facebook.com/groups/451858218222216/
3. Contact Susan Norwell who is an American educator, working on development of literacy in Rett Syndrome: https://www.facebook.com/susan.norwell?fref=pb_other
4. Watch this Webinar showing how fab Tobii eye tracker is, and how it will help you to evaluate the students, when they don’t know they are being assessed
Please feel free to contact me again via the Facebook pages, or on this site.
Best Wishes
Sally-Ann
Thanks for coming through on this, Sally-Ann! We are SO appreciative that you took the time to share these terrific resources!
Nancy, Whoops, I forgot to put in the link for the webinar about Tobii tracking software: Here is the link: https://www.youtube.com/watch?v=PZ3O5KcyiJw&feature=youtu.be
Feel free to contact me via my website: http://www.isletalkspeechandlanguagetherapy.co.uk/
I am working with a 10 month old girl who was just diagnosed with an extremely rare genetic disorder that mimics Retts in most characteristics but without the initial normal development. I am looking for advise on where to begin with an ACC intervention plan.
Robin, I am not sure if Theresa is still monitoring this post but I am happy to give my two cents. 🙂 In the absence of more information on the syndrome, I would just treat her like a beginning communicator with significant motor challenges. I’d probably consider heavy doses of aided language input by family and therapists with a PODD system to start. Switches would be great for play/entertainment at this young age. I’d start her on eye gaze, too. Lots to think about! Thanks for stopping by to comment.
I have been educating girls with Rett Syndrome for awhile now. I was recently transferred within my school district to be the “resource support” person for the girls included in the classroom setting and to teach the girls on hospital home bound (on home bound just because the parents were not seeing that the schools were teaching them appropriately.)
So far, this school year, I have been hitting a brick wall with the teachers and district staff members on the IEP teams. They do not believe my data on what the girl is capable of doing academically. They continue to undermine me and basically call me a liar.
I need some advice on how I can use research such as this article to explain that I am doing what is” best practice” for the girls. The schools just want to constantly test and asks questions to get data, which is creating a lot of anxiety, frustration and avoidance all together from my girls.
HELP Please…
Wow, that must be tough. I think many of us who provide supports to girls with Rett syndrome come up against this brick wall. It seems people either get Rett, and believe in the girls’ abilities, or they don’t get Rett, and are unable to see that the level of cognition cannot be proved because of dyspraxia.
I use eye gaze technology with them, and run a page on Facebook that you might find helpful: https://www.facebook.com/groups/451858218222216/
You would have to apply to join as it is a closed group. The page has a lot of files that you could read, and please feel free to copy and share the information.
Let me know if I can be of further assistance.
Sally-Ann
I work with a young girl with Rett Syndrome who has been very successful using eye gaze (fixation) to make choice and previously to answer simple questions or label. She has demonstrated some regression and is now inconsistent in her ability to look at pictures, she has cortical visual impairment, and has limited functional arm and hand movement to allow for tactile exploration. When she is alert and is using her vision she continues to use this successfully for communication, but I am looking for any recommendations for her communication on those days when she isn’t feel as well and is unable to visually attend. Thanks!